Alpha Prolipsis' Medical Services
Your reports will be available within 24 hours of receiving the sample
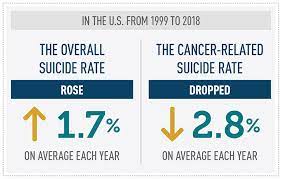
Battling cancer can exact a heavy physical, mental, and emotional toll on patients and their families. Even among survivors, multiple recent reports suggest, the course of the disease and its associated harms and stresses can significantly increase the risk of suicide.
One meta-analysis of 28 studies found that the suicide mortality rate among patients with cancer was nearly twice that of the general population. At highest risk were those with mesothelioma, pancreatic cancer, esophageal cancer, and liver and biliary system cancer.1 A separate study in Cancer that based its findings on the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) 18-registry database found that survivors of head and neck cancers had a 2-fold higher risk of dying by suicide than survivors of all other cancers.2
Why are head and neck cancers so prominent? “These cancers can be just utterly devastating to a patient’s quality of life,” says Jeremy D. Richmon, MD, associate professor of otolaryngology–head and neck surgery at Harvard Medical School in Boston, Massachusetts, who was not involved with either study. “The cancer tends to destroy how someone interacts with the world.”
In addition to significantly affecting the cosmetic appearance of many patients, a head and neck cancer can interfere with smell, taste, speech, swallowing, and other capabilities, “all of the basic functions of life that make us human,” Dr Richmon says. Those significant disruptions, in turn, can contribute to isolation, depression, and reclusiveness, all risk factors for suicide. If a patient does not have an adequate support system, he says, “it’s easy to see why this can become overwhelming.”
Researchers at the Pennsylvania State University College of Medicine in Hershey have similarly documented a higher incidence and prevalence of depression and other mental health disorders in patients with head and neck cancer.3 Coauthor Neerav Goyal, MD, MPH, an associate professor of otolaryngology–head and neck surgery and chief of the Division of Head and Neck Oncology and Surgery, says that the rate of mental health disorders in that patient subset increased substantially after their diagnosis and was significantly higher than in the general population.
Another recent Cancer study that likewise tapped the SEER database found that long-term childhood cancer survivors have an increased suicide risk as well, with male sex being an independent risk factor.4 A separate study in JAMA Oncology, again using the same national database, found that the incidence of suicide was significantly higher for patients undergoing surgery for 10 of the 15 cancers assessed in comparison with the general US population.5 At the top of the list were cancers of the larynx, cancers of the oral cavity and pharynx, and cancers of the esophagus. In this case, the cohort study found that patients who were male, White, and divorced or single had the highest risk of suicide.
Dr Goyal cautions that the existing instruments used to predict a patient’s risk of suicide are poor in sensitivity or specificity. In addition, he says that the Cancer and JAMA Oncology studies relied on the highly imperfect coding of medical charts to indicate that a patient had died from suicide. “So, it’s very likely that some of the markers that we’re looking at here are likely underestimated,” he says, adding that the underestimation probably occurred across the board.
One larger point from the various analyses and other published reviews, Dr Goyal says, is that patients who lack a good support structure seem to be at higher risk for depression, other mental health disorders, and, presumably, suicide. “Usually, that’s defined by patients who are divorced, single, don’t have kids, or don’t have family close by; sometimes it tends to be the older generation,” he says.
Smaller studies have backed many of the associations while adding further nuance to the overall findings. One recent report, for example, found that the risk of suicide is roughly equivalent with human papillomavirus (HPV)–independent and HPV-associated head and neck tumors.6 Dr Richmon, however, warns that different factors may be contributing to the risk for each group. The traditional group of patients with HPV-independent head and neck cancers tends to be older, have higher rates of tobacco and alcohol use, and carry other comorbidities. Although cancer may not be as much of an emotional jolt, it often carries a grim prognosis, and many of the patients, lacking robust support structures, are more vulnerable to mental health issues.
A separate cohort of patients with HPV-associated cancers tends to be younger and have fewer comorbidities. Despite a significantly better prognosis for many of their cancers, “it creates this cognitive dissonance between someone who’s in the prime of their life and has always been in great health and then suddenly has this cancer diagnosis and is considering a cancer treatment that can have significant side effects,” Dr Richmon says. “That shakes them, I think, more to the core and challenges their notions of mortality.”
Providers do not necessarily know at which point in the cancer treatment process a patient may be likeliest to die by suicide. Studies such as those by Dr Goyal’s group, however, have examined contributors such as depression and distress: They are easier to measure, and researchers can more easily gauge whether interventions are effective. “If we can do better from a depression standpoint then, hopefully, we can do better from a suicide standpoint,” Dr Richmon says.
“These cancers can be just utterly devastating to a patient’s quality of life. The cancer tends to destroy how someone interacts with the world.”–Jeremy D. Richmon, MD
The increasingly clear associations have led multiple research groups to urge earlier interventions to identify those at greatest risk. Madeline Li, MD, an associate professor of psychiatry at the University of Toronto in Ontario, Canada, recently joined a colleague in suggesting a “need to shift the clinical and research focus to the testing of proactive models of psychosocial care to improve mental health and prevent suicides in cancer.”7
At the Penn State Cancer Institute, Dr Goyal says, a care hub includes a psycho-oncologist who concentrates on the psychological needs of patients with oncological disorders, a social worker, a nutritionist, a financial counselor, and a chaplain. The growth of telehealth over the past few years has permitted the providers to increase their reach by holding more virtual meetings with patients, and this, Dr Goyal says, has had the added benefit of reducing some of the societal stigma around seeking help for mental health.
Not all hospitals and clinics have the same staffing and financial resources, however, and medicine is facing a severe shortage of mental health specialists. Even so, Dr Goyal says that validated patient surveys such as depression questionnaires and distress inventories can be readily administered by nurses. At Penn State, exceeding a threshold score prompts a visit with a social worker. “Having something that’s standardized, a short time burden, and easily deliverable allows physicians to have a barometer before they even walk in the room,” he says. That assessment, in turn, can help physicians to tailor conversations toward what is needed to help patients to reduce their distress or depression and, hopefully, reduce the risk of further harm.
Dr Richmon adds that patient-reported outcome measures assessing functional and emotional states, such as swallowing ability and mood, can similarly point out potential problem areas.
Although the recent studies have not provided easy answers, Dr Richmon says, they have at least shone a light on a troubling phenomenon. “Most importantly, there is much greater recognition that this is an issue,” he says. They also, perhaps, have offered a wakeup call for providers about the intertwined aspects of caring for a patient with cancer. “It’s not just curing the patient of cancer, but making sure that we optimize the patient’s health, functioning, and quality of life,” he says.