Alpha Prolipsis' Medical Services
Your reports will be available within 24 hours of receiving the sample
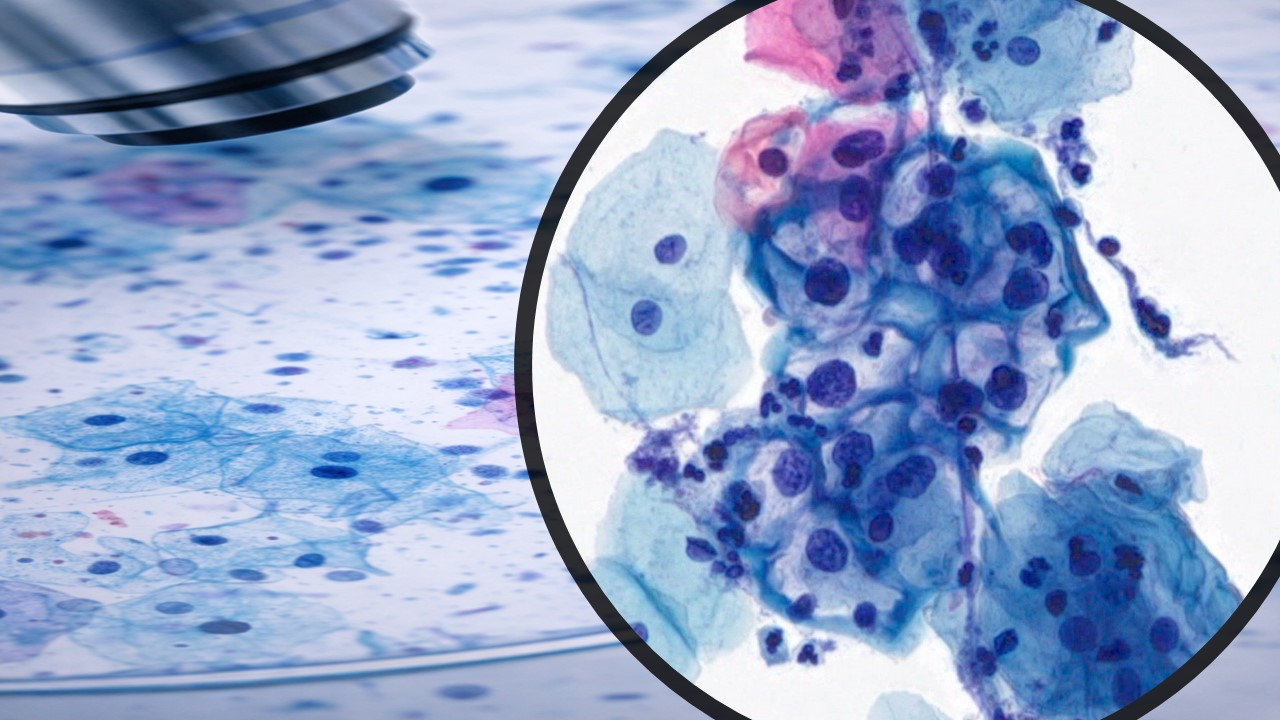
January 2024—The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is a widely endorsed and globally adapted standardized reporting system of thyroid fine-needle aspiration specimens. It has played a key role over the years in facilitating clear communication between cytopathologists and referring physicians on the diagnostic categorizations and in providing category-based risk of malignancy to help tailor personalized treatment strategies.
The first edition of this atlas, published in 2010, introduced a six-category tiered reporting system for thyroid FNA cytology, which remained unchanged in the second edition published in 2017. The aim of the recently published third edition (2023) is to provide a higher degree of granularity to the reporting system by incorporating unified terminology and eliminating duplication in diagnostic nomenclature.1 It focuses on aligning the Bethesda nomenclature with the recent 2022 World Health Organization Classification of Thyroid Neoplasms,2,3 further refining the category-based risk of malignancy estimates. In addition, it introduces cytology-based subcategorization of atypia of undetermined significance (AUS) and includes focused chapters on clinical perspectives, imaging studies, and the use of molecular and other ancillary tests.1
The six diagnostic categories (numbered I–VI) endorsed by TBSRTC are nondiagnostic (ND), benign, atypia of undetermined significance (AUS), follicular neoplasm (FN), suspicious for malignancy (SFM), and malignant. While a numerical designation continues to be incorporated, the TBSRTC recommends using the named diagnostic category as the primary method for reporting. Each reporting category in the new TBSRTC now has an updated and revised risk of malignancy, including the ROM in each category without noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). The new classification system acknowledges the limitations of the diagnostic category NIFTP while also providing a way to address it (Table 1).
A summary of the key updates within each diagnostic category follows:
Nondiagnostic. Previous editions of TBSRTC used the terms nondiagnostic and unsatisfactory interchangeably. The third edition recommends using nondiagnostic as the sole diagnostic term, emphasizing that while an unsatisfactory specimen is by default considered nondiagnostic, a technically satisfactory sample may also be categorized as nondiagnostic if cytologically it does not represent a specific diagnosis. Exceptions include aspirates with cytologic atypia, nodules with only inflammatory cells, and colloid nodules. Re-aspiration is advised for such nodules unless they are entirely cystic. TBSRTC, while acknowledging the controversy surrounding a quantitative minimum for sample adequacy, maintains the original adequacy criteria in the current edition and calls for more robust studies to provide further clarification in this area. Unlike prior editions, the third edition says there is no compelling evidence to delay a repeat thyroid FNA procedure by three months, as early repeat FNA has been shown to yield diagnostic material in up to 80 percent of cases.
FND: follicular nodular disease; AN: adenomatoid nodule; CN: colloid nodule; CLT: chronic lymphocytic (Hashimoto) thyroiditis; PTC: papillary thyroid carcinoma; HGFCDTC: high-grade follicular cell-derived thyroid carcinoma; MTC: medullary thyroid carcinoma; ANTC: anaplastic carcinoma; SCC: squamous cell carcinoma; NHL: non-Hodgkin lymphoma.
Benign. The updated TBSRTC recommends the use of follicular nodular disease (FND) as an umbrella diagnosis in cytology reporting instead of the benign follicular nodule terminology used in previous editions. Subclassifications like colloid nodule or Graves’ disease can be applied as needed based on cytomorphologic findings and clinical context. This recommendation is based on research indicating these nodules may or may not be clonal, suggesting a potential mixture of hyperplastic nodules and true adenomas in this category. FND is also well suited to cytology because these lesions have similar cytologic characteristics and since histologic distinctions (for example, solitary versus multiple nodules, encapsulated versus unencapsulated) are often unobservable in aspiration samples.
Atypia of undetermined significance (AUS). Studies performed post-introduction of TBSRTC have demonstrated notable variability in the use of AUS. Further stratification has shown an approximately twofold higher ROM in AUS cases with nuclear atypia compared with AUS cases with other types of atypia.1 To improve consistency and clarity in subsequent management, the 2023 edition recommends AUS as the preferred terminology, discontinuing the use of follicular lesion of undetermined significance (FLUS), previously considered an acceptable alternative for AUS. To align with the clinical risk and subsequent management, AUS is now subcategorized into two groups: AUS with nuclear atypia (referred to as cytologic atypia in the previous edition and raises a low level of concern for papillary carcinoma or NIFTP) and AUS–other with only architectural atypia. To further clarify: Thyroid aspirates that are limited by low cellularity, air-drying artifacts, blood interference, or excessive clotting artifacts should be categorized as either nondiagnostic or benign in the absence of genuine atypia and not as AUS.
Follicular neoplasm (FN). Like AUS, this diagnostic category is reported with great variability within the cytology community. In keeping with the principle of simplification of terminology, the 2023 edition endorses FN and discontinues the use of the prior terminology “suspicious for follicular neoplasm.” This is to avoid confusion with the next diagnostic category: “suspicious for malignancy.” In histology, the term FN corresponds with low-risk follicular thyroid neoplasms including NIFTP, thyroid tumors of unknown malignant potential, hyalinizing trabecular adenoma, and invasive encapsulated follicular variant of papillary thyroid carcinoma. With the intent of avoiding overtreatment of this group of follicular neoplasms, TBSRTC recommends limiting the use of FN to follicular-patterned neoplasms with subtle or focal nuclear atypia only. As a subgroup of FN, the oncocytic follicular neoplasm (FN-OFN) category is recommended for cellular aspirates that are almost exclusively composed of oncocytic cells. This distinction between FN and FN-OFN is important because these are genetically and morphologically distinct, raising different diagnostic considerations.
TBSRTC recognizes that the cytologic diagnosis of FN and FN-OFN may correspond to non-neoplastic lesions in histology such as nodular hyperplasia or lymphocytic (Hashimoto’s) thyroiditis. It therefore recommends using the following statement for clarity: “Although the cytologic features are in keeping with a follicular neoplasm, approximately 30 percent of cases diagnosed as follicular neoplasm (Bethesda IV) on FNA turn out to be benign follicular nodular disease on surgical resection.”
Suspicious for malignancy (SFM) and malignant (M). The SFM category is largely unchanged. In the malignant category, a few details have been included to correlate with the 2022 World Health Organization update on thyroid neoplasms.2,3 The term “papillary thyroid carcinoma, variants” is now changed to “papillary thyroid carcinoma, subtypes” to avoid confusion with the term “genetic variant(s),” which was based on molecular classification. The previously recognized subtype of papillary thyroid carcinoma, “cribriform morular variant,” is now designated as a separate tumor entity: cribriform morular carcinoma. The new term “high-grade follicular cell-derived thyroid carcinoma” is now also endorsed and replaces the older nomenclature of “poorly differentiated thyroid carcinoma.”
In conclusion, the third edition simplifies terminologies and harmonizes cytologic diagnostic categories with surgical pathology classifications. One recent study that examined AUS and FN subcategories demonstrated a significant distribution disparity, with 15 percent classified as AUS–nuclear atypia and 85 percent as AUS–other, prompting consideration of whether AUS–other could now become the new wastebasket category in the third edition.7 The study instead suggests exploring subclassification for FN nodules based on the presence or absence of PTC-like nuclear atypia.7 TBSRTC will continue to evolve as more studies assessing the impact of these updates become available.