Alpha Prolipsis' Medical Services
Your reports will be available within 24 hours of receiving the sample
ALPHA PROLIPSIS
NIPPLE ASPIRATION FLUID
Our goal is to provide accurate laboratory testing, with a reasonable turnaround time, in a cost-effective manner.
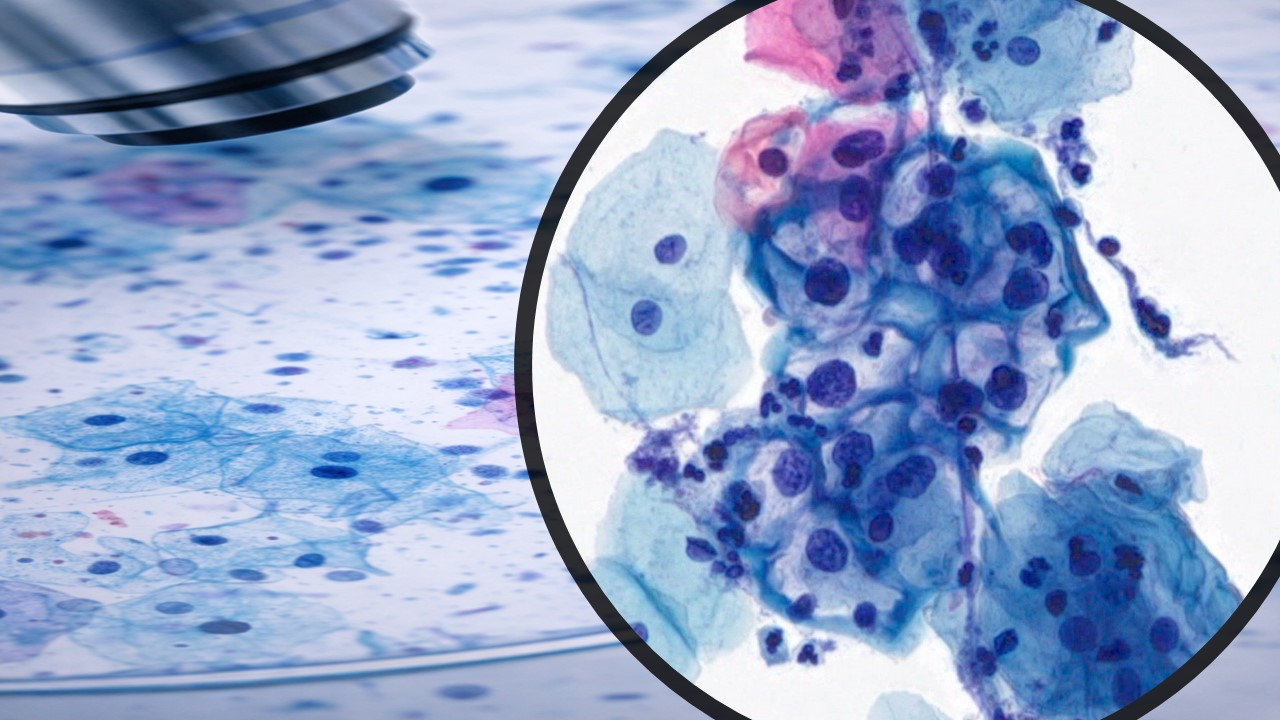
Fine needle aspiration cytology (FNAC)
Fine needle aspiration cytology (FNAC) has become popular as a valuable tool in preoperative assessment of breast masses, and it shows high accuracy, sensitivity, and specificity. It has gained popularity due to its fast and easy approach, being inexpensive, and can be performed with little complications. To differentiate benign from malignant lesions is one of the major goals of FNAC. In the evaluation of breast masses, the time honored triple assessment combines clinical, radiological, and pathological information, and FNAC, together with core needle biopsy, is the initial pathological investigative methods of choice. Much confidence has been placed on this approach for it can obviate standard excisional biopsy when all three components of the triple test are conclusively negative or positive
HALO is noninvasive, objective and repeatable, plus it's quick - just 5 minutes. It has been proven a safe and effective method to collect nipple aspirate fluid for analysis and a routine assessment with HALO will enable breast health monitoring and the ability to react to cellular changes early.
The HALO® Breast Cytological Evaluation Test is FDA approved for the collection of nipple aspirate fluid for cytological evaluation. The collected fluid can be used in the determination and/or differentiation of normal versus pre-malignant versus malignant cells.
Incorporating Halo into routine practice will enable physicians and patients to monitor cellular changes within breast ducts earlier, before they develop into larger, potentially cancerous lesions.
The HALO System is a simple, reliable method for NAF collection. NAF analysis is an objective assessment of a patient's breast health and can detect early warning signs of ductal cellular changes. Regular assessment and tracking of cellular changes in the milk ducts, where most breast cancer begins, enables clinicians and patients to take control of breast health.
The HALO Breast Cytological Evaluation Test is the only fully automated, noninvasive NAF collection system specifically designed for use in a busy primary care setting.
The HALO System provides important benefits to clinicians and patients:
For clinicians:
For patients:
HALO is not a diagnostic test and it cannot be used to exclude breast cancer. Patients should continue to undergo other clinical breast risk assistment procedures (mammography, clinical breast examination, self breast examination) as determined by and with their physicians.
Breast Discharge Cytoloqy: Nipple discharge. Label frosted end of slide with patient's LAST name with graphite pencil. Gently strip subareolar area and nipple with thumb and forefinger. When secretion occurs, allow pea-sized drop to accumulate on apex of nipple. Place slide on nipple and then draw slide quickly across nipple. Fix slide IMMEDIATELY with spray fixative or by immersion in 95% alcohol. Repeat procedure until discharge is depleted. If smears are prepared from both breasts, label each slide as left or right. Deliver in slide holders or jar with completed requisition to the Cytopathology Laboratory.
Health Tips
Do all breasts and nipples look and feel the same?
No, they don't. Breasts vary in size and shape, from very small to very large, very full or drooping. It’s common to have one breast that’s bigger than the other and sometimes this difference is noticeable.Breasts can feel different too, and the right breast can feel different to the left. Some women have lumpy breasts all the time, while others get lumpy breasts just before their period. Some have tender or painful breasts once in a while, others have breast pain all the time. Nipples look different too. They can be large or small, pale or dark in colour, stick out, lie flat on the breast or turn inwards.Women’s breasts change throughout their lives, for example when they’re pregnant, breastfeeding, gaining or losing weight, while they’re having periods and once their periods have stopped. Take a look at more information about breasts and being breast aware.
How do I check my breasts, and how often?
Once your breasts have developed, check them by looking and feeling. Do this regularly throughout your life. There’s no set time when to look and feel.There’s no specific way to check. Look at your breasts and feel them with any part of your hand or fingers. For example, some people prefer to use their fingertips, others the palm of their hand. Check all parts of your breast, your armpits and up to your collarbone.A mirror can help you look at the parts you can’t see easily. You may find body lotion or a soapy hand helps when you’re feeling your breasts.Get to know how your breasts usually look and feel. Then you’ll notice any unusual changes and feel more confident about going to your GP to get them checked.Men also need to be breast aware. In the UK around 350 men are diagnosed with breast cancer each year.
When should I have breast screening?
Women aged 50 to 70 are invited for breast screening every three years as part of a national screening programme. To be invited for screening you have to be registered with a GP.
You will get your first invitation between your 50th and 53rd birthday (in England the age range for screening is being extended to 47 to 73 as part of a trial in some areas, so your first invitation may come sooner than 50). You can contact your GP or local breast screening unit for more information.Women over 70 can continue to have a routine mammogram every three years. They will need to contact their GP or local breast unit to make an appointment. Between each screening mammogram, it’s important to continue to be breast aware and see your GP if you notice any unusual changes.
Why do my breasts feel tender and painful?
Breast pain is very common. It affects around two out of three pre-menopausal women at some point.There are two types of breast pain. Cyclical pain is associated with a woman’s periods, and usually happens for a week or so before a period. Non-cyclical pain can occur at any time, and can be there all the time. You can have pain in one or both breasts and you may describe it as a burning, prickling or stabbing feeling.There are practical things you can do to relieve breast pain, and drug treatments are available too. Find out more about breast pain and what can help.You could also try filling in a pain chart (you can find one in our Breast pain) to record when you get pain and how long it lasts for. It’s a useful record to show to your GP.
I’ve noticed a discharge from my nipple. Should I see my doctor?
You should see your GP if you have nipple discharge without squeezing your nipple. They may refer you to your local breast clinic.Nipple discharge in one or both breasts can happen for several reasons. Most women, especially if they’ve ever been pregnant, can squeeze some discharge out of their nipples. The discharge can be whitish, yellow-green or almost black. However, it’s not a good idea to squeeze your nipples.Nipple discharge is usually harmless. It’s most often due to a benign (not cancer) breast condition, such as duct ectasia or an intraductal papilloma, which may or may not need further treatment once it’s been diagnosed.Sometimes nipple discharge can be a symptom of breast cancer, particularly if it’s bloodstained.
I've found a lump in my breast. Should I see my doctor?
It’s important to get any breast lumps checked by your GP. They may refer you to your local breast clinic for more tests to find out what the lump is.Lumps in the breast are common and most are a symptom of a normal breast change or a benign (not cancer) breast condition.Lumps can occur at any time, though some are more common in certain age groups. For example, in younger women (aged 15-30) they are often fibroadenomas, while breast cysts are more common in women over 35 who haven’t reached the menopause.A lump in the breast, under the arm or near the collarbone can sometimes be a symptom of breast cancer.
What is a breast fine needle aspiration?
A breast fine needle aspiration (FNA) is a quick and simple procedure to perform, which removes some fluid or cells from a breast lesion or cyst (a lump, sore or swelling) with a fine needle similar to a blood sample needle. The sample of fluid or cells is smeared on a glass slide and sent to a pathology laboratory to be examined by a specialist doctor (a cytologist) under a microscope. An FNA is performed to help determine the nature or diagnosis of the lesion and to plan treatment if necessary.
Breast FNA may also be used to aspirate a cyst (that is, using the needle to draw fluid from the cyst)to remove it completely or relieve discomfort if the cyst is large and tender.
If the lesion cannot be felt from the surface of the skin, the doctor may use guidance for the FNA by using ultrasound images or pictures (see ultrasound). This shows an image of the inside of your breast on a screen to allow the doctor to ensure the needle is going into the lesion. Alternatively, this can be done under stereotactic (mammography) guidance if the lesion has only shown up on a mammogram.
How do I prepare for a breast FNA?
There is no need for special preparation before a Breast FNA. Breast FNA can be done immediately after you have had a medical examination and any imaging your doctor may have referred you for, such as a mammogram and/or ultrasound to find out the cause of the lesion.
Breast FNA can be uncomfortable and sometimes painful and you may wish to ask a friend or a relative to attend the appointment with you if you think you will need some support before or after the procedure.
Wear a comfortable two piece outfit, as you will need to have the upper body undressed for the Breast FNA.
What happens during a breast FNA?
The doctor performing the breast FNA will decide whether it is best to use ultrasound or mammography images or pictures to locate the lesion and guide placement of the needle. If the doctor can feel the lesion it is said to be “palpable”, and these are sometimes sampled without using imaging to guide the needle.
Ultrasound guidance
You will be lying on your back on the examination bed in the ultrasound room, the upper body undressed, with one arm above your head on the pillow in a comfortable position. The doctor will put a clear gel on your breast and the ultrasound transducer or probe (see ultrasound) will be slowly moved across the breast to show and identify the lesion on the ultrasound screen. The doctor will clean your breast with an antiseptic liquid and place the needle through the skin and into the lesion guided by the ultrasound images.
Local anaesthetic on the skin area where the needle is inserted is sometimes given. If the doctor does not provide anaesthetic you can ask about this before the needle is inserted.
When the needle is inserted into the lesion, the doctor will make several small (less than 1cm) forward and backward, gentle movements with the needle to collect cells or, if the lesion is a cyst, fluid may be collected. Two or three separate samples are usually taken in this way to ensure a good sample has been obtained.
Mammogram guidance
If the lesion is too small to feel and cannot be located with ultrasound, you may need mammography to find the lesion and help the radiologist direct the needle into the lesion to get a sample of tissue
It is much more common for mammographic biopsies to be core biopsies (see breast core biopsy) rather than FNA. The procedures are generally very similar.
You may be sitting up or lying face down for Breast FNA depending on the equipment that is used. After the needle is placed into the breast, the radiographer will take mammograms to check the correct positioning of the needle within the lesion before the sample is taken.
Are there any after effects of a breast FNA?
Breast FNA can be uncomfortable and sometimes painful. Local anaesthetic is sometimes used and can be requested if needed. Any pain after FNA can be relieved with non-prescription analgesics like paracetamol. You should not take aspirin because this thins the blood and may increase bleeding and bruising.
Minimal bleeding or bruising can appear after the procedure, especially if you are taking anticoagulant medication (aspirin, warfarin or Plavix). Breast FNA does not leave a scar on the skin.
There is no significant risk of infection as a result of FNA. A small proportion of women feel faint during FNA but this generally passes quite quickly after the test has finished. A pneumothorax (perforation of the space around the lung by the biopsy needle with collapse of the lung) is extremely rare.
How long does a breast FNA take?
Breast FNA is a quick test, which takes 10 to 20 seconds for each sample and this procedure may be repeated several times until the doctor is sure a good sample is collected. The examination and FNA procedure will generally take around 20 to 30 minutes for ultrasound guidance and 45-60 minutes for mammographic guidance.
What are the risks of a breast FNA?
The risks of a breast FNA are rare and minimal and can include:
Minimal bleeding and bruising, especially for those on anticoagulation (warfarin, heparin), aspirin, or anti-platelet medication.
Risk of infection is rare. Breast FNA is a clean and sterile procedure, which uses skin antiseptic and disposable one-use needles.
Breast implant perforation can happen if the lesion is close to the implant but is a rare complication using ultrasound or stereotactic (mammography) guidance.
Pneumothorax (perforation of the lung cover by the needle with lung collapse) is an extremely rare but serious complication that is more frequent if the lesion is deeply located in a small breast.
If the lesion being biopsied is found to be cancer, there is a very small risk of displacement (“seeding” or implantation) of tumour cells along the tract or path of the needle as it is withdrawn from the breast. This is extremely rare.
Breast FNA may not always provide a definitive diagnosis (or answer) about what the lesion in your breast is. In particular, it may not allow cancer to be definitely ruled out even if no cancer cells are found in the samples of material removed from your breast. The result of the FNA needs to be considered along with the results of other breast imaging and your doctor’s examination findings.
Breast FNA is not 100% accurate. The results must always be interpreted by the doctors caring for you in the context of the findings of your breast imaging (mammogram and/or ultrasound), pathology results of the tissue or fluid sample and the findings of a medical examination. This is called the “triple test”.
What are the benefits of a breast FNA?
Breast FNA is a quick and simple procedure to perform to investigate a breast lesion.
There are few complications in having the test and few cases where the test is not appropriate due to a pre-existing medical or physical condition. Breast FNA can be used when other needle biopsy procedures are not possible, for example, if you are using anticoagulant medication, have an allergy to anaesthetic, or have a breast implant.
Who does the breast FNA?
Breast FNA should be done after careful medical examination and imaging tests such as mammogram or ultrasound as part of the “triple test” to ensure the correct diagnosis is made. Breast FNA is done by specialist doctors experienced in breast needle biopsy procedures.
Where is a breast FNA done?
Breast FNA is an outpatient procedure. Image guided breast FNA will be performed in a public or private hospital, radiology practice, a public or private specialist breast clinic, at a BreastScreen assessment clinic, or a surgeon or doctors’ rooms equipped with ultrasound.
When can I expect the results of my breast FNA?
Tests of the fluid or tissue sample will need to be done in a laboratory to confirm the diagnosis and are usually available within one or two days. These results, together with the results of medical and imaging examinations, are considered and interpreted and a report written for your referring doctor. Usually, you can obtain the final results of the breast FNA from your own doctor within a week.