Alpha Prolipsis' Medical Services
Your reports will be available within 24 hours of receiving the sample
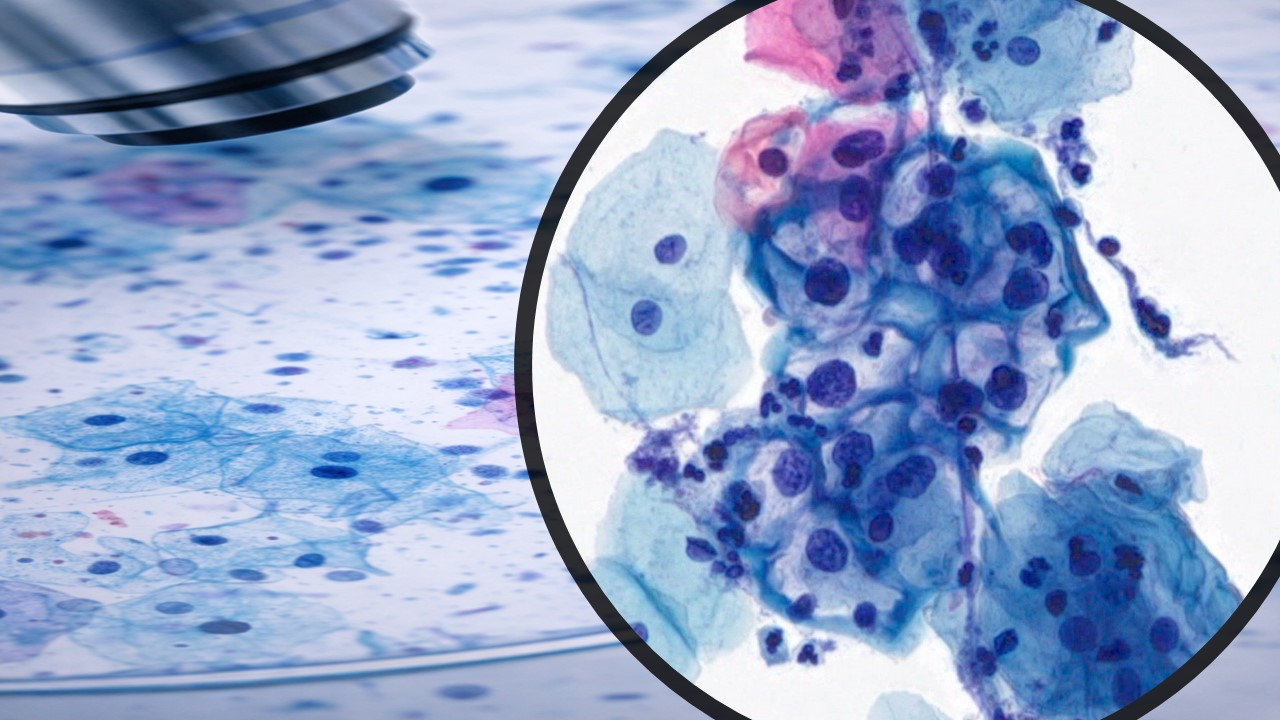
January 2024—Urinary cytology is widely used to screen for high-grade urothelial carcinoma (HGUC) and to monitor for recurrence. Several reporting systems have been proposed over the past few decades, but The Paris System (TPS) for Reporting Urinary Cytology is the most widely applied worldwide. The first edition of TPS (TPS 1.0) was published in 2016,1 and the second edition (TPS 2.0) was published in 2022.2 TPS focuses on accurately identifying HGUC and reducing indeterminate diagnoses. TPS 2.0 revises some diagnostic criteria, modifies diagnostic categories, updates the risk of malignancy (ROM) for each category based on data, and develops management recommendations.

The sensitivity of TPS varies between 37.5 percent and 93.6 percent, with a specificity range of 73 percent to 100 percent. The positive predictive value falls between 62.3 percent and 100 percent; the negative predictive value ranges from 46 percent to 96.5 percent. The overall diagnostic accuracy is reported at 82.8 percent. Much of this variability depends on the patient population and how many samples from patients with hematuria are being screened for HGUC versus patients with a known history undergoing routine monitoring. Cell block material can be helpful in a subset of cases, particularly those with large, three-dimensional clusters that are better visualized on tissue section; however, TPS 2.0 makes no comment on criteria that should be applied to cell blocks. In addition, molecular tests may increase accuracy in certain scenarios.
Adequacy. Adequacy is essential to assess in all cytology specimens. Urine cytology adequacy data remains scant, however, and TPS 2.0 is essentially unchanged from TPS 1.0. Adequacy criteria for voided urine are greater than 25 mL with ThinPrep and greater than 30 mL with SurePath preparation,2 and for instrumented urine greater than 20 cells/10 high-power fields.2 Instrumented urine with 10–20 cells/10 HPF is classified as satisfactory but limited by low cellularity.2
Diagnostic categories. While the emphasis of identifying HGUC remains the same, some changes were made to the diagnostic categories and criteria of TPS 2.0. Notable updates have been introduced in the negative for high-grade urothelial carcinoma (NHGUC) category. This includes a refined discussion on atypical versus benign-appearing urothelial tissue fragments and the integration of insights into low-grade urothelial neoplasms (LGUN), which was previously addressed in a standalone chapter in TPS 1.0. Additionally, the new version provides a more comprehensive characterization of degenerative changes in benign specimens, emphasizing the importance of not making abnormal diagnoses based solely on the presence of degenerated cells.
TPS 2.0 recommends an elevated threshold for degenerated atypical urothelial cells (AUC) when only degenerated AUCs are observed. Furthermore, the guidance highlights that HGUC cells tend to be discohesive, and it is generally more beneficial to examine singly dispersed cells in a specimen for atypia rather than focus solely on tissue fragments. These updates collectively contribute to a more nuanced and precise approach in urine cytology interpretation.
The diagnostic criteria for AUC include one major criterion (nuclear-to-cytoplasmic [N/C] ratio between 0.5 and 0.7) and one of three minor criteria (nuclear hyperchromasia; irregular nuclear membranes; and irregular, coarse, clumped chromatin).2 The diagnostic criteria for suspicious for high-grade urothelial carcinoma (SHGUC) includes the major criteria (N/C ratio ≥ 0.7) and two of three features (moderate to severe hyperchromasia, irregular clumpy chromatin, and irregular nuclear membrane).2 Diagnostic criteria for HGUC include N/C ratio ≥ 0.7, hyperchromasia, irregular nuclear membranes, coarse/clumped chromatin, cellular pleomorphisms, prominent nucleoli, mitoses, necrosis, etc. The nuclear area is a more critical cytomorphological criterion than the N/C ratio for HGUC cell detection, for which digital pathology and artificial intelligence may be helpful. A subset of HGUC shows hypochromasia, which is also supported by digital image analysis.
Furthermore, a new chapter focused on upper urinary tract (UUT) cytology explores the challenges involved. A digital image study demonstrated that UUT HGUCs have higher N/C ratios, smaller cell circumference, smaller nuclei, and less cytoplasm compared with the lower urinary tract (LUT).3 A cutoff range of at least five to 10 abnormal cells for LUT specimens and ≥ 10 cells for the UUT specimens was originally recommended for making a diagnosis of HGUC in TPS 1.0. The thought process was that diagnosing HGUC with fewer than five diagnostic cells would lower the risk of high-grade malignancy (ROHM).4 However, TPS 2.0 makes note that there is insufficient data specifically addressing the issue of quantitation. As a result, a strict cutoff distinguishing SHGUC from positive for HGUC cannot be supported. TPS 2.0 states that SHGUC should contain “few” diagnostic cells while positive for HGUC should contain “many” diagnostic cells. In instances where the number of diagnostic cells is limited, the determination to label a diagnosis as positive for HGUC should consider not only the severity of atypia exhibited by all abnormal cells but also the clinical context and specimen type. Furthermore, while not essential for the diagnosis, additional features that may be observed include eccentric nuclei, prominent nucleoli, necrosis, pleomorphism, mitoses, and apoptotic bodies. Finally, the frequency of each diagnostic category is extremely variable and again depends primarily on the patient population: 0.3–3.6 percent nondiagnostic (ND), 50.5–90.5 percent NHGUC, 1.2–23 percent AUC, 0.2–6.6 percent SHGUC, 1.9–14.1 percent HGUC, and 0.1 percent other malignancies.
As mentioned, the low-grade urothelial neoplasm category is abolished, and LGUN is included in the negative for high-grade urothelial carcinoma category.2 As a result, there is an increase in the false-negative rate and ROM in NHGUC.5 However, recent studies on urine cytology for LGUN with TPS 2.0 criteria demonstrated low sensitivity (21.7 percent) and high specificity (97.2 percent) with a positive predictive value of 87.5 percent, negative predictive value of 58.6 percent, and accuracy of 61.9 percent, providing justification to no longer recognize LGUN as a separate diagnostic category.6
Risk of high-grade malignancy. TPS 2.0 highlights the utility of urine cytology as identifying clinically significant cancers, particularly HGUC, and chooses the term ROHM rather than ROM, which was used in TPS 1.0. In a new chapter, the ROHM for each diagnostic category and ROHM-guided clinical management are discussed. ROHM is 0.0–17.7 percent for ND, 4.8–36.8 percent for NHGUC, 12.3–66.7 percent for AUC, 33.3–100 percent for SHGUC, 58.8–100.0 percent for HGUC, and 12.5 percent for the LGUN diagnostic categories. Based on the ROHM of each diagnostic category, the clinical management for each diagnostic category was detailed.
Summary. We strongly endorse applying TPS 2.0 recommendations, which include several updates from TPS 1.0, to evaluate urine cytology. Implementation of TPS has standardized the diagnostic criteria, thus limiting interobserver variability in cytologic interpretation, creating a more reproducible diagnostic tool and improving communication between clinicians and cytopathologists.