Alpha Prolipsis' Medical Services
Your reports will be available within 24 hours of receiving the sample
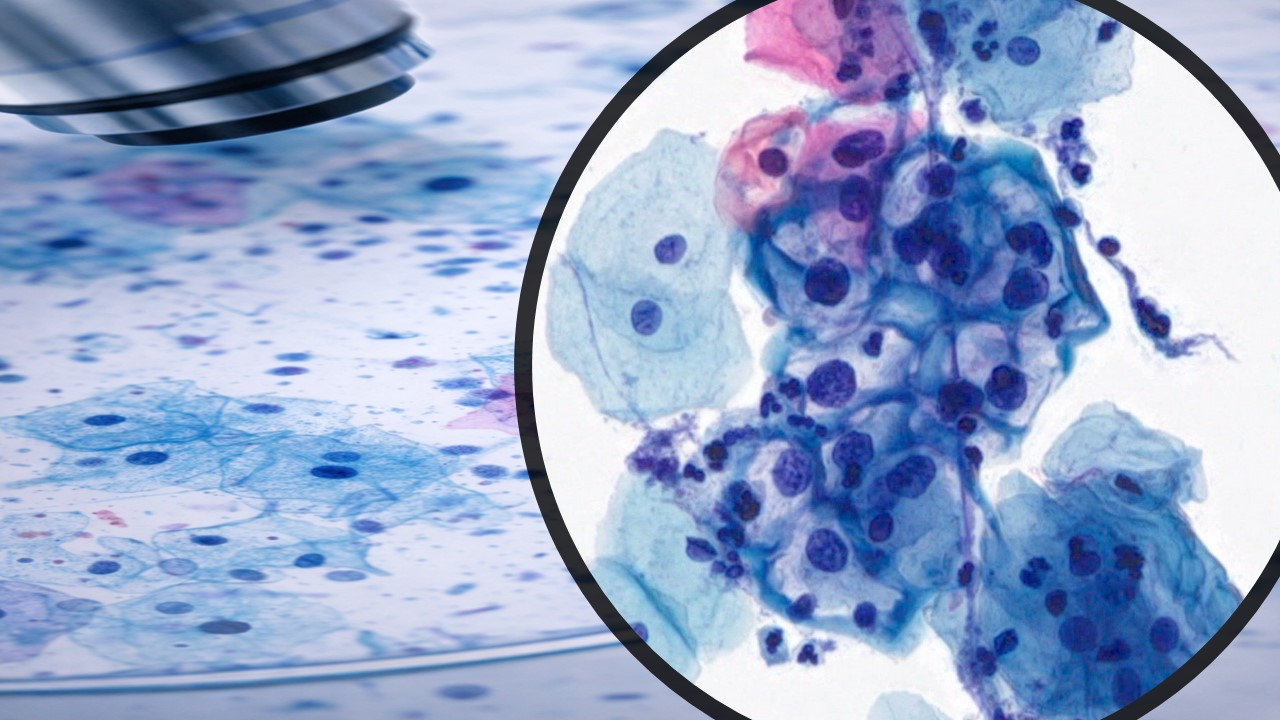
n a recent article published in Nature Medicine, researchers assessed the harms, benefits, and affordability of seven primary screening algorithms for human papillomavirus (HPV) in the general population of women across 78 lower-middle-income countries (LMICs) using the Policy1-Cervix platform.
These screening algorithms were i) primary visual inspection with acetic acid (VIA); ii) primary cytology with HPV triage; iii) primary HPV without triage; iv) primary HPV 16/18 triage; v) primary HPV VIA triage; vi) primary HPV colposcopy triage; vi) cytology; vii) primary HPV cytology triage.
The World Health Organization (WHO) Guidelines Development Group has found all these potentially suitable for LMICs.
The Policy1-Cervix platform models HPV transmission, vaccination, HPV type-specific natural history, cervical cancer screening, diagnosis, and treatment.
It also simulates persistent HPV infection, which can progress to cervical intraepithelial neoplasia (CIN) grades I, II, and III. Notably, CIN 3 can progress to invasive cervical cancer over time.
This platform has been extensively validated against data from various countries; thus, it captures screening management algorithms in detail, including downstream management of HPV+ women, pre-cancer treatment, and surveillance after colposcopy.
Per the WHO cervical cancer screening and treatment guidelines published in 2021, the general population of women in LMICs should undergo primary HPV screening in a screen-and-treat or screen-triage-and-treat approach on turning 30 years.
Further, they recommended repeating this screening every 5 or 10 years onwards. The study findings would help inform these WHO guidelines.
In the present study, researchers performed modeled evaluation over a three-stage process. First, considering multiple screening frequencies and ages, they evaluated the advantages and losses (pre-cancer treatments proxied losses) of all seven algorithms.
Next, they evaluated adverse obstetric outcomes caused by pre-cancer treatments, another measure of the losses associated with cervical cancer screening, and affordability outcomes.
Lastly, they explored the optimal management of women after negative triage tests and pre-cancer treatment.
They presented the results of all three phases to the Guidelines Development Group in July, September, and November 2020.
For mutual consensus on key parameters and assumptions, the research team regularly met with the WHO guidelines development group members and relevant technical teams.
They also discussed the interpretation of the results attained. Notably, the team only considered those screening and triage technologies for which there was an adequate evidence base to support modeling.
Screening intervals for primary VIA and cytology in the base case were three and five years, respectively, while for primary HPV screening, these intervals were five and ten years.
In the normative analysis, the researchers assumed that 70% and 90% of women attended each routine screen and adhered to follow-up or treatment, respectively.
Finally, the team reported the cost and affordability of each outcome, including reduction in cervical cancer incidence and mortality, the number of pre-cancer treatments needed to prevent death (NNT), the incremental cost-effectiveness ratio (ICER), reported as US dollars per Healthy-Adjusted Life-Year (HALY) saved, and pre-term delivery events associated with pre-cancer treatment.
In comparison, screening algorithms involving triaging women pre-treatment with 16/18 genotyping, cytology, VIA, or colposcopy had nearly comparable effectiveness as fewer pre-cancer treatments and HPV screening without triage.
However, HPV screening with VIA/cytology every three years was less effective and affordable compared to HPV screening every five years. Furthermore, the VIA method led to more than double the number of pre-cancer treatments than HPV.
Considering 70% coverage, primary HPV screening strategies were the most effective and affordable, reducing cervical cancer age-standardized mortality rates by 63–67% when offered every five years.
To conclude, primary HPV screening is the most effective and affordable cervical cancer screening option in LMICs.
This WHO elimination strategy could potentially prevent more than 62 million deaths in LMICs over the next 100 years. Thus, the study findings support the 2021 WHO cervical cancer screening and treatment guidelines.